Collaborative Care Team in Open Source,
Issues and Approaches
Draft Version 6.5, 10 May 2011, Etienne Saliez
- Summary:
- In the scope of the ISfTeH,
what are the specific issues of telemedicine, out of the large
domain of medical informatics?
- A review of issues and considered approaches, with the
following questions:
- How far are the issues well identified ? Which issues are
still missing ?
- Assuming agreements on an issues, which approaches should be
considered ?
- Identified Issues:
- Main issues:
- Issues:
- The trend is that many specialised actors become necessary
for the
care of the same patient and the needed expertise is not available
everywhere. Since 50 years many excellent specialities have been
developed, but the
coordination has been relatively neglected.
- Telecommunications could help more, but are still underused.
- Too many custom softwares. Up to now most softwares did
focus on only one target group
of users at a time, one professional specialisation, or one disease, or
one context.
- Good healthcare is not yet enough available nor affordable in
developing regions. A critical concern in the scope of the ISFTeH, the
members coming from about 50 countries, including many developing
regions.
- A more detailed analysis of the issues is presented in the
next chapters of this overview of issues.
- Approaches:
- Objectives:
- Improved care by means of better support of collaborations
between the professional
actors in charge of the care of a patient, by means of telemedicine and
sharing know-how in the scope of the ISfTeH, International Society of
Telemedcine, http://www.isft.net/
and http://www.isft.net/cms/index.php?collaborative-care-team-in-open-source
.
The essential concept of telemedicine is seen 2 or more healthcare
partners having to collaborate, even when there are not at the same
location.
The project focus on a "patient-centric multidisciplinary
record". A
record belonging to the patient in which the involved care providers
can share information.
- Sustainability by means of education, seen here as
contextual training.
- A kind of
health coordination platform, beginning by the most common features for
the care process, as it may be necessary for any kind of
diseases, for any kind of healthcare professionals, in any kind of
context. This common platform is intended to integrate additional
specialised software modules.
- To share know-how, including full documentation in Open
Source.
- Experimental prototypes in order to:
- Stimulate constructive discussions with the intended users,
in front of visual examples.
- Check the feasibility of the considered up to date
technologies.
- Care Team Concept:
- Issues:
- The traditional organisation was based on many independent
and individualistic
practices and independent hospital departments. These
organisations did
more and more specialise, looking each at only one or a few aspects of
the patient problems.
- Since the development of
very much larger medical knowledge bases, no one is any more able to
cover in depth all the aspect of medicine.
- A patient could always have more than one problem at a time.
- Up to now many commercial softwares have been designed to
make life easier to a specific target group of customers, either GP, or
nurses, or cardiologists, or hospital administrators, or.... or ....
with limited motivations about interoperability.
- Initially when internet was not yet available, most medical
record softwares
have been designed as "personal computers". The
consequence is that these different groups of professional users have
still today completely independent
software designs, with poor compatibility.
- Approaches:
- In the scope of the ISfTeH, a new reflexion about how
to improve healthcare, taking advantage of telecommunications tools.
- The start point is the generic concept of "Multidisciplinary
Collaborative Care
team", i.e. all the care providers involved in the care of a common
patient. An overview of the patient situation should always be shared
by all
members
of the care team. Next depending on their professional profiles
care
team members may have different roles, going deeper in their specific
domains.
- Care Team members are expected to share information in a way
intended to be easily understood by care team
colleagues.
This is why a problem list must be maintained. Indeed any new
member of the Care Team, for example in an emergency unit, should
always find an up to date overview of the problems as the first page.
- Care Team coordination:
- Normally the long term coordination is expected to be
achieved at the Primary Care level, by the GP. He is motivated
for follow-up and he should normally receive reports from the diverse
specialists.
- When necessary the GP may delegate a problem to a
specialist,
as well temporarily the coordination during admissions in hospitals.
- The concept of care team can be implemented in many ways, as
long as several partners have to collaborate for the same patient. A
few examples in case of:
- Oncology: GP discovering the problem, organ
specialist analyzing the exact situation, surgery, radiotherapy,
chemotherapy, home care, ....
- Diabetes: GP, diabetologist, vascular diseases,
ophtalmologist, ...
- Developing region: nurse in the village, regional hospital,
center of excellence, international experts.
- Elderly care: follow-up by the GP, multiple disabilities
which may need specialists, care at home.
- Pathology lab: local surgery taking a sample, lab
technician preparing images and providing a provisional conclusion,
remote expert providing a second opinion.
- ....
- Problem solving:
- Issues:
- Up to now many medical archives, as well on paper as well on
electronic media, contain essentially descriptive and narrative
data. Events, like consultations and admissions, are described as
separate
reports. Many medical records systems contain a lot of raw
data, but often lack any synthesis of
the problems.
- Many regions have a great shortage of experienced healthcare
staff, particularly in developing regions. Remote small
health centers must relay on persons having
relatively short nursing education.
- Some advanced decision support system already exist, but are
not yet largely available. Standardization of the observations remains
a major issue.
- Approaches:
- Since the essential healthcare goal is to contribute to solve
problems, we should go beyond simple narrative documentation.
Today informatics technology makes a more rigorous information
management possible.
- Medical "work methodology":
- Collaborations in a Care Team require agreements about how
to manage and to share patient information.
- Clear guidelines are particularly important for beginners.
- Orderly managed patient information is a prerequisite
before access to medical knowledge bases would become useful.
- Orderly managed information is always a factor of care
quality. It prevent that some issues would be forgotten and
neglected.
- Also a prerequisite before advanced decision support could
be implemented in the future.
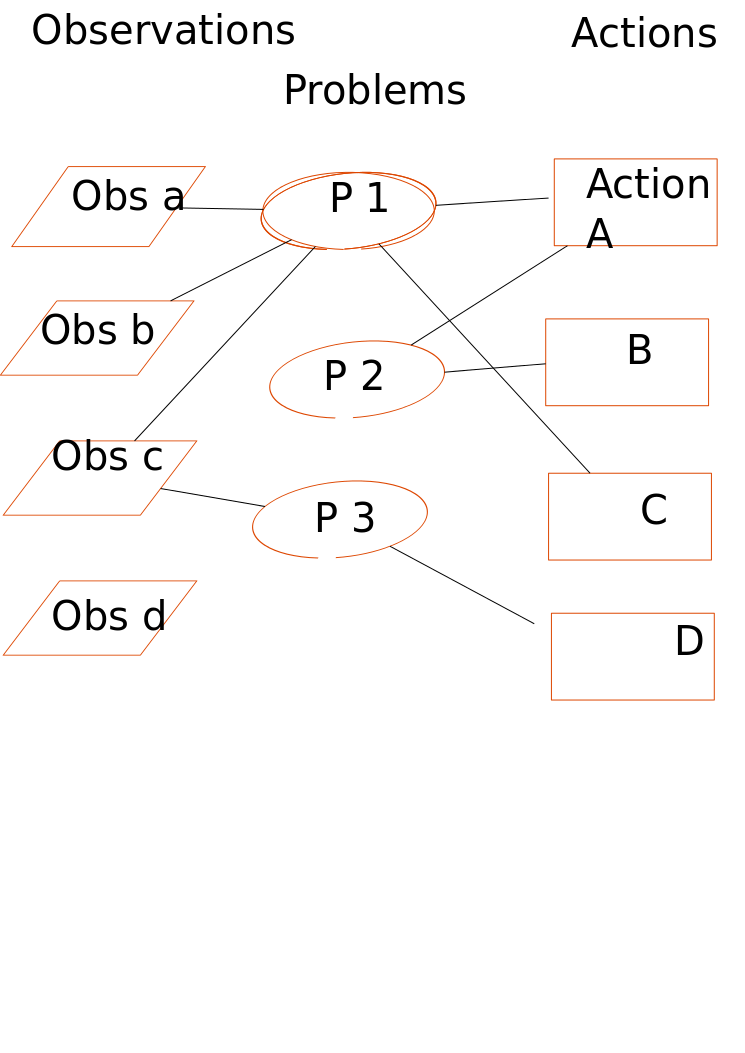
- The recommended approach is to make at least clear
distinctions between
Observations, Problems and Activities and to pay attention to the links
between these 3 types of informations.
- Observations:
- Record the facts, as what the patient did say, what you
did see, what has been measured, etc... Take notes about what is
obvious and should initially be token without any assumptions.
Beginners can learn relatively
quickly how to take notes about observations.
- Health Issues assessments:
- Given the available observations, assessments will be
made
about one or more health issues. Heath Issues may be preliminary
concerns about a set of abnormal finding. May later become a
diagnose. Health Issue include also risk factors.
- All care provider whatever they roles, should have a
minimum of overview of the problem list. Of course depending on
their specialised roles, will go deeper in the details of their domain.
- Activities:
- Decision about activities are based on the current
understanding of the Health Issues by the doctor, often not yet any
obvious diagnose but just provisional hypothesis.
In the future some Activities will become automatically proposed on the
basis of the current Health Issues so far identified. For example
which next questions to the patient, or which test seems to have the
highest priority, on the basis of what is already known as possible
Health Issues.
- Activities include a wide range of possible procedures,
as well intended for more explorations, as well for treatments.
- Since Activities necessitate resources, they have to be
declared to the administration who need to make invoices.
- In principle all activities will result in some kind of
conclusion, as e.g. a lab report or a note about the effect of a
treatment.
These results will increment the above set of Observations and may
introduce a next iteration of assessments and new activities.
- Schemas:
- Semantic web technologies will be here very useful in order
to represent:
- Inside the patient record, the links between Observed
facts, identified Health Issues and ordered Activities.
- Links fro the patient problems to external medical
knowledge bases.
- A basic example: Obs-Problems-Actions.png,
- Information Flexibility
and Navigation:
- Issues:
- Up to now many software applications are not going deeper
than handling "documents" and forms, regardless of the meaning of their
content. For example discharge letters are archived as a 2 or 3
pages document in free text. Structured information are limited
to patient ID, date, author, ICD diagnose code.
- Like paper charts most electronic archives are organized as
trees. Typical main usual branches are consultation notes,
discharge letters, general lab, bacteriology lab, pathology lab, XRays,
... A given document, or leave in hte tree, has only one access
path.
- Approaches:
- Items:
- No more large documents nor rigid "forms", but
much more granularity in smaller entities
of information. An Item is in general the minimal entity of
information making sense, technically speaking an "object" with several
"attributes".
- A much more granular approach become necessary. The basic
unit of information can be defined as an item, .i.e. an object with a
few attributes as
- Item Header:
- Item ID, and version, Date, Time, Subject of care,
Responsible author, Link to the Context (e.g. during a given
consultation at
a given location and time).
- Item Type (Observation, Issue, Activity) and subtypes.
- Optional Clinical Modifiers, as degree of belief,
intensity, optional comments.
- Item content:
- Depending on the type.
- Moreover a collection of Items may be represented by
means of an Item.
- Different types of content may have different
methods of display.
- Navigation:
- No more a tree structure, but possible access by multiple
"paths".
- The
use of "Semantic Web" technologies is considered, in order to manage
navigation between
- The Items of medical information inside the patient
record.
- Links to medical knowledge bases.
- Graphical representation of the links between knowledge
nodes.
- Clicking on a node in order to provide the details of the
underlying information.
- The links themselves should be qualified too, with author,
date, degree of belief, etc... i.e. the links themselves could be seen
as Items.
- "Views":
- Polymorphic collections, list of medical Items relevant for
a given objective, but regardless of their technical formats.
- Frequent search strategies should be facilitated by means
of sets of rules recorded as preferences, in general as well as
individual preferences.
- Education:
- Issues:
- Helping a few individual patients is of course an urgent
need, but the main challenge of emerging countries is to provide
sustainability.
- Approaches:
- Beginners need above all to learn how to manage medical
information. This is why the above method of explicit recording
of "Observations-Problems-Activities" is particularly recommended for
beginners.
- Access to textbooks of theoretical knowledge must be
available, however it
is not enough because the lecture of textbooks is arduous.
- Education is to learn how to solve problems. As far as
possible a transparency of the decision steps is very important, as
explained above. Semantic schemas will be probably more easy to
understand than long explanations in text.
- Scenario of "Contextual
training":
- Ask local staff to record what they have observed,
- Ask them to document their current understanding of the
patient problems,
- On their request provide a second opinion:
- If in agreement, a motivating acknowledgement for the
local staff.
- If suggestions to proceed in a different way, a factor of
training, when providing some background information related to the
current
Health Issues. Maybe just one page of explantions.
Next time a similar situation will arise, the local staff is expected
to
know better how
to proceed.
- User guide of the system itself:
- Also by means of contextual explanations, when clicking on
help buttons included in most pages. The user guides may depend
on
the user preferences in function of the level of training.
- Applications
Integration Platform:
- Issues:
- In the past many custom softwares have been developed
independently, due to the following factors:
- The members of care teams have different roles, different
professional interests and different preferences.
- Internet was not yet easily available.
- Healthcare professionals were not too much motivated for
collaborative work.
- Software commercial companies were not at all interested in
interoperability, unless forced to do something.
- Many specialized medical application softwares are already
available as
FLOSS, as can be seen on http://www.medfloss.org/
, but there is not much coordination between these initiatives.
- Approaches:
- An integration platform is seen as a critical need.
- Modularity:
- Modularity is critical in order to allow distributed
developments. A key
issue in order to take advantage of distributed development in an
international community in open source. Partners should take care
of development and maintenance of components.
- There are 2 main types of software components:
- ( A ) Availability of the common functionalities,
as
expected
necessary in most care contexts:
- Most critical as the "Core" of the network and implying
agreements.
- Main components:
- User authentication and authorizations
- Patient identification
- Role Based Access control
- A generic structure of Observations - Health Issues -
Activities,
- "View" steering objects,
- Normalized interface to knowledge sources
- ... more information at http://www.chos-wg.eu/Software/Comp-Common-Platform.html
.
- ( B ) Interfaces to many specialized services:
- Interface definitions is here particularly important.
- Beside the interface itself, there should be as few
dependencies as possible, between the platform and the external
modules.
- Since these components could be available in different
programming languages, the interfaces should be neutral as far as
possible, sharing information in XML.
- The integration platform will:
- Call external "services"
- Could also be called by external process,
particularly be
notified of the occurrence of external events.
- User preferences:
- User preferences are important in order to take account of
the different role of user roles in the care team. Keep in mind
that an important goal of the project is to avoid multiplications of
custom softwares.
- Users may need specific screen presentations and
behaviours,
depending on professional profile, specializations, cultural context,
spoken language, computer experience level (beginners learning basic
skills or seasoned users wanting to work as fast as possible),
etc... as well in function of individual preferences.
- User preference should be associated with user accounts,
allowing users to move to several workstations.
- To keep it easy many preferences should be proposed
automatically when a user account is created with the main information
classes as professional status, specialization, role in organization,
membership in a care units, etc...
- There are 2 types of user attributes:
- Mandatory attributes, to be managed by the network
administrator in function of legal and organisational
requirements.
In read-only mode for the user.
- Optional preferences to be managed by the user.
- Communication strategy:
- Issues:
- Electronic messages did replace traditional postal
services. The improvement is that it works faster, but it
remains depending on the good will of a sender. Moreover the
sender cannot exactly know who would need which information in the
future.
- A message is
a kind of picture at a given point in time and become quickly
obsolete. What if the patient would need care by a new Care Team
member, as an emergency department ? and what if the treatment
has just been modified one day ago?
- Approaches:
- On-line access to shared information is considered to provide
the best support
for collaborations between the Care Team members.
- Any new information should be recorded
directly in the patient record. In that way any authorized member
of the Care
Team can get it immediately. Even a new member who has just been
added in the Care Team.
- That said the possibility to receive and to send messages
must remain available. However the trend will be to reduce
message to "notifications". A notification is a kind of short
message warning the addressee to pay attention at some new information
relevant for him and already located in a given patient record in the
database. Such notifications will contain just a pointer and no
more any medical
content.
For example when the result of a bacteriology test become available
after about a day, the lab will at the same time make the result
available in the patient record and send a notification to the author
of the request.
- Confidentiality:
- Issues:
- Confidentiality is critical for the patient. Although
in principle all care providers have always an obligation of
confidentiality, the question is to avoid unnecessary risks.
- Confidentiality between doctors may sometimes be an issue
too.
- Approaches:
- Role Based Access Control principle, i.e. access to the
patient record must be limited to the actors who are currently really
necessary
for his
care and who have the agreement of the patient.
- Explicit care Team management, i.e. a short list of who
exactly in charge of the patient. At one side new
Care Team members can be invited by persons who are already Care Team
members, as well by the
patient himself. At the other side the patient could
occasionally let remove a
member.
Anyhow Care Team memberships are of limited duration, only during a
meaningful delay after the
latest contact.
- The
new vision implies much more transparency between the
healthcare professionals. For the benefit of the patient, care
providers, when in charge of the same patient, should share all
relevant information. However when there is no common patient,
information do not need to be shared except for scientific purposes and
then in an anonymous way. This is good for both the patient
privacy, as well for potential competition issues between care
providers.
- Trust and responsibilities:
- Issues:
- Information of unknown origin could not be trusted.
- Different actors
could have sometimes different valuable opinions about the same set of
observations.
- Legal requirement of traceability.
- Approaches:
- In order to add new information, the user must be be
qualified and accredited as a member of the care team of the
patient. For example a prescription depend on 2 conditions: be
given by a doctor who is currently member of the Care Team. For
example the pharmacist chosen by the patient is considered as a
temporary member of the Care Team.
- Any member of the Care Team may introduce comments, but the
responsible author must always remain visible.
- The computer network is neutral and different medical
opinions are allowed to be
recorded alongside, always mentioning the responsible author.
- Someone else than the original author should be able to
express his opinion,
approving or disagreeing. The system must be able to record this
kind of "co-signature"
of the
original document. The point is here to prevent Care Team
colleagues to create unnecessary new copies of the same documents.
- Versioning:
- Update of Items are normally never allowed, but only new
versions. This should be true for all Items, even including
the patient identification.
- For medical reason it may be important to be able to go
back to a previous step.
- Also a mandatory legal requirement. A decision is
acceptable according the "rules of the arts" in function of all what
was known at the time of that decision.
- Technical collaborations, FLOSS:
- Issues:
- Many specialized medical services are available as FLOSS, but
integration is still far from obvious.
- Keep in mind that informatics is an evolutive process with
request for new versions and new applications, as well with the
discovery of new tools.
- Approaches:
- Remark: the full name is normally "Free Libre and Open Source
Software", but
is often abbreviated as "FLOSS" or "Open Source".
- Promotion of technical collaborations based on FLOSS
principles, sharing software know-how according to the principle of the
GPL, http://www.gnu.org/licenses/gpl.html
. or related licences as the EUPL, http://www.osor.eu/eupl
, taking account of the European context and legally available in 22
languages.
- An international community of informaticians supported by not
for profit organizations.
- In order to make developments possible across such
distributed centers, modularity is a critical issue.
- Incremental developments makes possible to start early with a
minimum, to learn from field experience and to improve one component at
at
time. A complete planning in advance would take too much time and
would become soon obsolete.
Trying to anticipate a little, an initial vision is proposed, but many
details will have to be worked out, and the main vision itself will
have
probably to be adapted in the future.
- Maintenance:
- As for any softwares, open source softwares need long term
maintenance, which need to be managed. While in general never
licences costs, support services may need to be charged.
- Software architecture:
- Issues:
- The main objective of the project is patient care. A
patient may need care from a very large panel of specialized services,
requiring an
integration platform.
- To make distributed developments possible.
- The logic of the intended medical applications require a
relatively large set of temporary persistent information. More
information than just a few data about the next HTML page to be
displayed, as usual in many web frameworks.
- The general philosophy should be real time and measures
should
be foreseen in order to prevent conflicts in case that 2 users would be
working on the same record.
- Approaches:
- A very modular approach:
- A "Core" intended as a generic integration platform.
- As far as possible reuse of software components available
in Open Source and adapted as "services". Interfaces allowing
that these external component may be in different programming languages.
- The Core itself is also a component to be upgraded step by
step, although particularly critical. The Core of the
experimental prototype is in Python. A choice in function of a
good level of abstraction, a great flexibility, availability of large
libraries and a growing and a mostly open source minded community.
- Incremental development beginning by relatively simple
components, to be upgraded one at a time.
- A compromise between a traditional application logic and a
stateless web framework. This can be seen as 2 levels:
- Core Patient Record Coordination Logic. A multi-user
setup, but during a user session, maintenance of a Session object
containing temporary session data related to the current user.
Every user should have such a session object. Session objects
should be maintained on a fast type of memory.
- Front-end web interface dealing with all the external
communications, in principle called "views". The most frequent
views are
intended for a web browser, but other types of "views" should also
foreseen in the front-end, as smart phones, HL7 messages exchanges,
etc...
- .... more information at http://www.chos-wg.eu/Tech/VCT-Network-Architecture.html
.
- Network installations:
- Problem:
- In telemedicine it would be very difficult to go to visit all
users on site for installation and maintenance purposes. This is
particularly critical in the case of developing regions.
- Phones are
already largely available in developing regions, where budgets for more
complete workstations are very limited.
- In developing regions power supply and internet are not
always continuously available 24
hours a day.
- Large centralized servers rise potential problems from
ethical and
political
points of views.
- Approaches:
- "Thin client":
- The user workstation should be as simple as possible.
- The essential requirement is to be limited to a standard
browser as
available on most usual OS platforms. A
browser based on full open W3C standards should be required, if
possible.
- Although a standard web browser is currently seen as the
main
technology,
we will also have to take account of other devices, as phone devices.
- In general no options should depend on the client machine,
but well on hte user account at the server side.
- Servers:
- Servers are intended to do all the work.
- Network configuration:
- Decentralization:
- Avoid unnecessary centralization of data bases.
Preference for relatively small regional servers, while a possibility
of long distances inter-connexions must be available. This can be
better controlled since it applies to only a small percentage
of the patients. Server should be decentralized at regional level in
the region were the patients are living. The degree of
decentralization may depend on several factors as where are cluster of
frequent transactions expected, where is basic technical maintenance
and
protection possible.
- Servers need to be interconnected, in order to get access
to remote medical expertise and in case a patient would need care at an
other location than his usual region where he is normally living.
- Confidentiality control is easier when the number of
transaction is relatively limited.
- Autonomy:
- Workstations and servers should include a battery
maintaining a stable power for at least some time.
- Server and client could be in the same machine, although
this kind of extreme decentralization is only intended for back-up or
emergency situations when no communications at all are available.
- Access to the international Internet is mandatory, even if
it use need to be limited due to high costs and porr continuity:
- Necessary to get support from remote medical expertise,
otherwise not available locally.
- Mandatory for occasional software maintenance.
- Network security:
- Issues:
- Security:
- Security is a major concern for confidentiality,
but above all for the reliability of the applications. Indeed orders
for treatments need to be safely transmitted.
- Security require attention at both sides of the
communication,
server and client. A problem is that it is relatively difficult
to
control the security at the client side. For example passwords should
not be saved.
- Remark: the possible goal is only a high degree of
security, higher than what was possible with papers and manual
signatures.
- Reliability:
- Integrity of the information.
- Data availability:
- Medical emergencies can arise at any time 24 hours a day,
and access to the
patient record could be important.
- Telecommunications could be interrupted at any time for
some time
up to several hour or a few days, particularly in developing regions.
- Any machine could fail at any time.
- Approaches:
- All communications must be encrypted. Current
technologies are based on HTTPS.
- In principle only a minimum of information should go through
the communication channel.
- Identification of the user session, by means of a kind of
cookies, moreover very temporary and if possible somehow encrypted.
- Of course the requested data to be displayed and new input
as which button has been pressed and new input
data.
- Communications must be encrypted. Moreover the traffic
on the line should be limited to
what is really essential, i.e. identification of the client (maybe a
kind cookie) and what is new. For security reasons, systems
based on steering information in long URLs should be avoided.
- Sensitive information should not unnecessary depend on slow
and potentially unreliable telecommunications between server and
workstation. Session information should be maintained at the
server side.
- Checksums or signatures should be included in critical
information.
- Automated backup must be foreseen, not depending on the
attention of local users:
- Backup on several devices.
- Incremental backups.
- In situations where communication are very difficult, it
could even be considered to keep backup at the workstation level,
regarding the most critical information for the surrounding patients.
- Information
Interoperability:
- Issues:
- Official "standards" did contribute to alleviate the
interoperability problems. However only to a limited extend since
proprietary softwares companies are always trying to avoid to
expose how they
work internally.
- Historically standard have been designed mainly for
epidemiological purposes. Clinical modifiers, which are mandatory
in care practice, are not yet well standardized.
- Standards defined
many years ago in very different contexts are not necessarily a panacea
for
our current purposes.
- Approaches:
- Of course when useful, use official standards, but we may
need more.
- Open Source is expected to become a major factor of
interoperability.
- References to dictionaries should be systematically prefixed,
with worldwide unique prefix.
- While classifications of academic diagnoses are very well
standardised, as for example the ICD from the WHO, more should be
developed in the domain of "Heath Issues" concepts and links to related
knowledge.
- Data collection for statistics:
- Issues:
- Misunderstandings are frequent. There are 2 very
valuable
groups of objectives, but be aware that they may require different
strategies:
- ( A ) Surveys for scientific and management goals:
- Historically the first application did focus more or less
exclusively on this type of objectives.
- ( B ) Patient care:
- Individual patient care application were developed at a
later stage.
- Approaches:
- ( A ) Surveys:
- Information must here be made anonymous as far as possible.
- Detailed information from groups of more or less similar
cases need to be reduced and summarised in classes, by means of
standard codes as the "IDC" from the WHO. What matter here here
is conclusions about large populations, within acceptable error margins.
- The current classifications focus on final academic
diagnoses, but more attention should be devoted to "Health
Issues". From a management point of view "Health Issues" may
require resources, even when a suspected diagnose has been eventually
excluded.
- Many healthcare professionals are not motivated for surveys
and would need incentives before participating seriously in surveys.
- The registration of classifications and codes should be
made very easy. As far as possible the information should be
automatically derived from the clinical practice. In many obvious cases
the user would only have to give one validation click on the proposed
classification.
- Anonymous information could also be used for quality
control purposes.
- ( B ) Patient care:
- Reliable patient identifications are here critical.
- Detailed information is here absolutely necessary in order
to arrive at meaningful decisions. "Clinical Modifiers" are
essential, as degree of belief, acquisition reliability, intensity,
frequency, duration, laterality, etc... In clinical practice
these important aspects are usually communicated in free text, or even
by means of movements and voice tones.
- In telemedicine the challenge is now to make all these
important information available to partners in the Care Team, who may
be at remote locations. The
challenge is to achieve more reliable clinical information sharing,
while
keeping the system easy to use. The most important clinical
modifiers should begin to be normalized, while free text comment should
remain possible everywhere.
- Economics of medical activities:
- Issues:
- In general the tradition is that doctors are paid when they
encounter patients, face to face. Historically Social Security systems
have been build on that principle.
- Developing regions have a major "brain drain" problem.
Even
in regions where national doctors could be available, there are 2
problems:
- Attraction to migrate to
countries where incomes are higher.
- Isolation from continued learning opportunities.
- Approaches:
- Seek agreements about fees, based on services and
responsibilities through internet, making the face to face contact no
more mandatory.
- Telecommunications and access to knowledge can alleviate the
isolation in remote areas.
- To a limited extend experts are available and agreeing to
give advices as volunteers, but:
- Take care that the questions should be well prepared and
documented.
- Volunteers should have no out of pocket expenses about
equipment and internet access.
- Beside pure medical applications, provide software tools
helping to manage the related administrative issues including invoices.
- Developments management:
- Issues:
- Too many local software projects are reinventing more or less
the same things.
- Approaches:
- An international collaborating community.
- Official status:
- Currently a Working Group of the ISfTeH:
- In the future an independent legal status could become
necessary:
- A kind on international not for profit association:
- Could be a Belgium based AISBL-IVZW, "Association
Internationale Sans But Lucratif" or "Internationale Vereniging Zonder
Winstoogmerk", http://www.ejustice.just.fgov.be/cgi_vzw/vzw.pl
:
- Like an ordinary ASBL-VZW, Belgian not for profit
Association, but adapted for an international context:
- Members do not need to be Belgian nationals.
- Basic obligations include a postal address in
Belgium, publication of the statutes, a yearly report showing that the
association remain really non profit.
- More in the book http://www.uga.be/uitgeverij/detail_fr.phtml?id=678
.
- ...
- Still remaining an affiliated member of the ISfTeH.
- Version control systems:
- A decentralized version control system, like Mercurial, http://mercurial.selenic.com/,
or Bazaar, http://bazaar.canonical.com/en/
.
- Every partner get locally a full documentation of the
projects.
- Temporary local branches are allowed and may include any
local initiatives. However of course integration in one or a few
main version branches are strongly recommended, in the interest of
everybody.
- Discussion tools:
- Voice, text, images,
- Preference for using Open Source tools as: .....
- Documentation:
- A web site and a forum keeping the reports from the
discussions.
- ....
- Exploitation management:
- Issues:
- Making software available is not enough.
- Users need support services for installation, initial
training, help desk in case of problem.
- As any software, open source software need evolutive
maintenance.
- Approaches:
- Management of maintenance for the projects in production:
- IPATH:
- .....................
- ......
- Support service of Open Source softwares are seen as a
traditional business.
- More issues should be covered ........
{kind=link}